


Johnmoses Washington was well into a 29-year prison sentence when one of his worst fears was realized. He got hurt.
Incarcerated at 17, Washington grew up in state Department of Corrections prisons. He had heard the stories, seen the pained men limping their way through their time. Then the socket surrounding his left eye was shattered.
“My eye and my face didn't feel right, and it didn't even look right,” Washington said. “You could look at my face and tell that something was wrong.”
So he did what prisoners do when they need help — he filed a “kite,” a note requesting medical attention — and then he did the next thing they do. He waited.
As days turned into weeks, Washington’s eye slowly crept deeper inside his skull. His orbital bone, misaligned at the fracture, began to knit wrong. Two months passed before prison medical staff sent Washington to a hospital for surgery. Because of the delay, bone and muscle had to be pulled from his hip to stop his eye’s retreat.
“It's par for the course, unfortunately, for those who are incarcerated,” said Washington, who was released on July 8, 2019 after serving 21 years in prison. There is, he said, “a belief that prisoners deserve and need to go through pain and anguish.”
Prisoner accounts laid out in lawsuits, investigations from a new watchdog office and internal department documents obtained by Crosscut point to a pattern of delay that leaves the state’s 18,800 incarcerated men and women unable to access basic health services.
Homicides and suicides in prison may draw more focus, but, in Washington as in much of the country, nine out of 10 prisoners who die inside fall to illness. And, though many are lifers, about a third of those who don’t leave prison alive are dead before they turn 55.
When complaints rise about medical care provided through the Department of Corrections, blame often falls on cost controls meant to ensure the department doesn’t blow its whole $1.1 billion annual budget on health services. But in interviews, more than a dozen current and former inmates, their families and their advocates argue the department maintains a culture of callousness.
As critics tell it, incarcerated people struggle to get basic medications and supports like wheelchairs and walkers. Former inmates describe prisoners with protruding hernias and crippling chronic injuries that could be repaired with simple surgeries, but are left to fester. Now, even as the department attempts to navigate the pandemic without a permanent head of medical services, officials wonder what the coronavirus and the coming austere state budgets will bring.

Prisoners walk toward an exercise yard at the Washington Corrections Center in Shelton, Aug. 31, 2015. (Ted S. Warren/AP)
In a recent interview, Deputy Secretary Julie Martin acknowledged challenges facing the Corrections Department’s health system and noted several recent reforms. While recruiting and retention of skilled medical staff have proved a stubborn problem, Martin, a process-oriented efficiency expert who joined the Corrections Department in 2014, evinced pride in the nurses and doctors working with patients who sometimes arrive in prison with unaddressed chronic illnesses and no medical records.
“If it were myself, let's say, going in there … I would feel pretty confident that we're providing good health care,” said Martin, the department’s No. 2 administrator, who has also been the acting head of health services since early March.
“I don't think any of us would say we're providing the health care that we would love to provide to everybody, and there's numerous reasons for that. … We have room to improve what we do, but I don't think that I'd necessarily be frightened,” she said.
Spending continues to climb both because of the overall increase in the cost of health services and the graying population within Washington prisons. With a month to go in the fiscal year, that cost has already broken last year’s record and reached an all-time high of $183 million.
The department has pledged to spend what it must to meet its obligations to provide “medically necessary” care to incarcerated individuals. “All needed nondiscretionary medical care is provided, regardless of funding levels, which often requires DOC to find funds from other budget streams,” said spokesperson Janelle Guthrie, using the abbreviation the department is commonly known by.

A room used for recreation by inmates in solitary confinement at the Washington Corrections Center in Shelton. (Ted S. Warren/AP)
A lower standard
Describing the provision of health care inside a prison as an uncommon challenge, Guthrie said the department “aspires to community-level quality of care and strives to ensure that the standard of care meets the requirements” set in state law and by U.S. Supreme Court precedent.
J.W. Gamble was serving his time on a Texas penal farm in the fall of 1973 when a 600-pound cotton bale fell on him, wrenching his back. Months passed as prison officials gave him pain pills and, when he refused to work, punishment before Gamble received care. The lawsuit Gamble filed ended up before the Supreme Court and, in 1976, set the standard for health care in American prisons.
It is not a high bar.
Mistreatment or a lack of treatment does not violate the Constitution’s ban on cruel and unusual punishment unless the failures are intentional. Care that may constitute medical malpractice outside does not within a prison’s walls. Poor medical care driven by negligence, rather than intent, is constitutional.
In Washington and elsewhere, prisons have settled on providing only the care they deem necessary for a prisoner to survive without losing basic life skills, like bathing. Prisoners can still serve their time with a useless shoulder or bulging hernia.
Correctional health care, like much of prison life, edges up against a maxim shared by prison administrators and their critics: The time is the punishment.
“The punishment is going to prison, not what happens to you in prison,” said Dr. Marc Stern, a correctional health care expert based in Washington state. “If the judge didn't sentence you to death, the prison doesn't have a right to provide such poor health care that you die.”
Stern went to work at the Department of Corrections in 2002 and found a “decentralized system of health care run by superintendents” at each of the system’s prisons. By the time Stern left the department in 2008, he had crafted the health care management framework that exists today. He described it as a “work in progress” about which he “had no regrets.”
“I was glad we did it,” Stern said. “We were making improvements, and I think it needed to continue to be refined, as does anything else.”
Recent changes in policy allow the department medical director to overrule the standards set in the health plan. Frontline providers told by an oversight board that they can’t provide medications or treatments were also recently provided the ability to appeal those denials.
Critics of the system would like to see a great deal more refinement, if not a total overhaul.
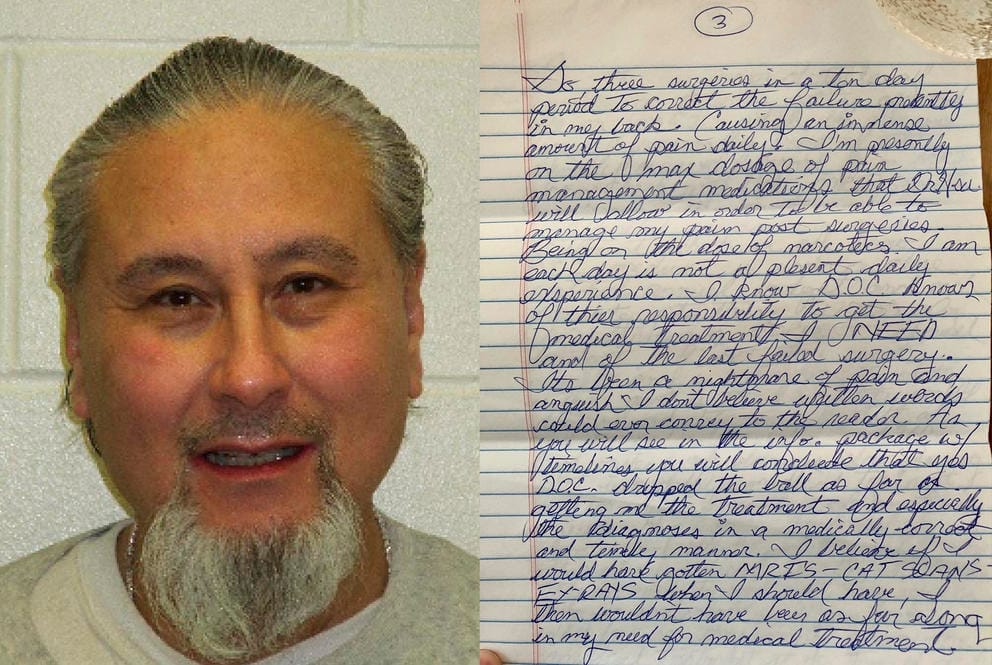
Incarcerated since 2007, Michael Sublett has complained about back pain from a 2016 back surgery in which metal rods placed in his back began to fall apart almost immediately. “It’s been a nightmare of pain and anguish,” he wrote in a 14-page handwritten letter detailing his treatment. (Washington Department of Corrections; Michael Sublett)
The Tylenol cycle
Medical issues have been the top concern inmates offer to most organizations that take their complaints, including the 2-year-old Office of Corrections Ombuds, the state’s first independent oversight body monitoring the prison system.
Restrictions inside the department’s health plan contribute to delays that sometimes hurt and kill incarcerated people, said Nick Allen, a staff attorney with Columbia Legal Services, a Seattle nonprofit law firm active on corrections issues.
There is, Allen said, a pattern. Sick and injured inmates are given Tylenol or another over-the-counter drug. When that cure fails, the inmates receive physical therapy or another treatment that doesn’t require a higher level review, before returning to the Tylenol. Those who make it to a specialist often see recommendations ignored.
“It was just insanity to watch how they would continue these people on this cycle and never just go to the solution that was right in front of them,” Allen said.
Guthrie noted new initiatives meant to increase the quality and speed of care. The department, she said, is working on ways to enable staff to more rapidly address any lapses, and it is lobbying the Legislature to pay for a larger medical staff.
Incarceration itself complicates everything. Medical staff have difficulty developing rapport with their patients, with whom, Guthrie said, “every interaction takes place in alignment with the roles within the criminal justice system.” But, she argued, some inmates receive better care inside prison than they ever had access to outside.
"Many come into incarceration with underlying, untreated medical conditions we are able to help address while they are incarcerated,” Guthrie said by email. “That said, DOC is always working to improve care, find efficiencies and ensure that resources are being directed towards the highest priority areas.”

Washington's prison population has become older since the 1990s, as convictions for violent crime are not eligible for early release and as an aging generation grows. (Elaine Thompson/AP)
A question of necessity
The department’s priorities often diverge from those of the women and men in its care. Common, debilitating ailments go unaddressed because treatment, by the prisons’ standards, is not medically necessary.
One inmate with a hernia that caused him daily pain could not get surgery because treating his injury was not necessary in the department’s calculus. In a court declaration, he recounted crying as he tried to push the hernia back in during a visit with his wife; he worried the visit would be cut short if he called for help. Another described medical staff denying surgery to remove objects embedded in his temple even though he struggled to eat, sleep or walk, while a man who struggled to breathe after his nose was badly broken said the department refused to pay for a specialist to examine him.
In a deposition filed with U.S. District Court, a physician treating one prisoner with ulcerative colitis, an inflammatory bowel disease, recounted asking to conduct a biopsy to confirm the diagnosis. The doctor’s request was denied and, as he feared, the man’s colon ruptured through his abdominal wall and nearly killed him.
“This is not how you treat human beings,” said Allen, who led the failed class action lawsuit in which those stories were collected.
“A lot of this stuff has life or death implications,” he continued. “If you're not taking it seriously, if you're treating folks as ‘other,’ that's going to result in unnecessary and preventable death.”
If not death, then pain.
Incarcerated since 2007, Michael Sublett has served nearly all his time in grinding pain. A decades-old motorcycle injury that flared not long after he arrived at Washington Corrections Center in Shelton has left him unable to walk. A “marathon” 8½ hour back surgery performed in 2016 left him worse off than ever, Sublett said. Spacers placed between his vertebrae attached to two, 10-inch metal rods near his spine began to painfully fail almost immediately.
“I lay in bed and screamed for more than three hours before anyone came to my aid,” said Sublett, describing the night seven months after surgery that the screws failed.
“It’s been a nightmare of pain and anguish,” he continued in a 14-page handwritten letter detailing his treatment.
Sublett said he spent years begging prison medical providers to allow him to have his back examined. When the scans were ultimately conducted, Sublett said by letter, doctors at Providence St. Mary’s Medical Center in Walla Walla found that his spine had collapsed, and that four of 10 screws had failed.
Currently receiving bone strengthening treatment at UW Medical Center, Sublett said he expects to undergo three surgeries to correct the failed attempt to fix his back. The 61-year-old credited Dr. Sara Kariko, the department’s chief medical officer, with personally intervening in his case to get him the corrective surgery he has needed for nearly four years.
In a recent interview, Kariko said “there is always room for improvement” within the department’s medical system. But, she argued, many prison care providers see themselves as advocates for “underserved and vulnerable populations” and pursue the work passionately.
Sublett relies on a wheelchair, a device that prison staff can take away from him at any time. He may never walk again, he said, and faces the prospect of becoming quadriplegic in prison.
“I am incarcerated to pay for crimes against society,” said Sublett, who was sentenced to life without parole under Washington’s “three strikes” law after being convicted of murdering a Thurston County man. “I was not sentenced to be physically and mentally punished for over a decade with debilitating pain.”
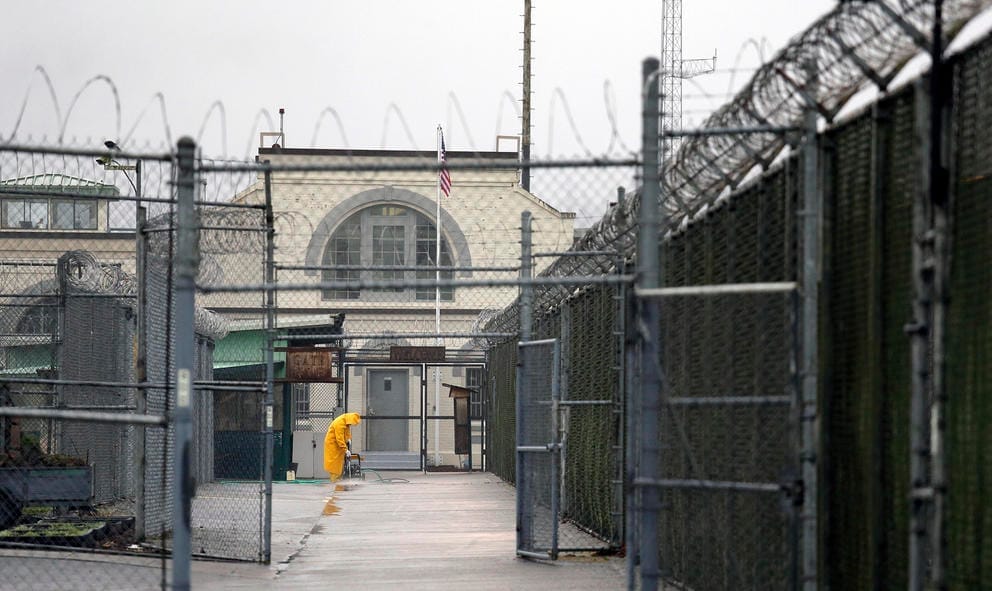
A man does maintenance work between razor wire-topped fences at the Monroe Correctional Complex in Snohomish County. Inmates at the prison filed a motion in April with the Washington state Supreme Court asking it to order Gov. Jay Inslee and Department of Corrections Secretary Stephen Sinclair to release inmates who are 60 years old or older, those with underlying health conditions and any who are close to their release date. The motion came after almost a dozen people at the prison tested positive for the new coronavirus. (Elaine Thompson/AP)
For families, fear
The coronavirus, having killed two prisoners and infected 315 others in Washington, threatens to burn through state prisons, as it has in institutions around the country. Columbia Legal Services' Allen said the department's history provides little cause for hope.
“They can't provide adequate medical care just on a regular normal day during normal times, and you really expect them to be able to appropriately treat people while a pandemic is going on?” Allen asked.
Columbia Legal Services and others petitioned the state Supreme Court to speed the release of prisoners and take additional steps to contain the virus. The Supreme Court turned them down during an April hearing.
“We were devastated that the Supreme Court did what they did,” said Suzanne Cook, chair of the Department of Corrections family council. “The result of it is DOC will continue in the manner in which they have.”
Cook takes a dim view toward the department’s “manner,” and says the department’s medical system has nearly killed her husband several times.
As she describes it, Cook spends most of her time bird dogging her husband Darrell’s medical care. Darrell Cook, convicted in the mid-1990s of rape and, separately, murder, has seen his health falter and, Suzanne Cook said, he nearly died after falling into anaphylactic shock due to an emergent allergy. The steroid regimen that followed almost took his life as well.
“He lost 30 pounds in two months,” she said. “His body was dying, and they were canceling appointments.”
Darrell Cook’s health had stabilized under the care of a new medical director at Monroe Correctional Complex, the prison system’s medical hub. The complex fell into controversy in early 2019 when it became known that seven inmates there had died because of apparent mismanagement by Dr. Julia Barnett. Barnett was fired and is being investigated by state health authorities.
Suzanne Cook had become, if not optimistic, confident that her husband of 15 years wouldn’t die of his now well-documented illnesses while under Dr. Areig Awad’s care. In June, though, Darrell Cook was transferred to Washington State Penitentiary in Walla Walla, where the 62-year-old’s spate of near-fatal episodes began.
The move means Suzanne Cook must begin her cycle of advocacy again to make sure her husband gets medication for his heart condition and insulin for his diabetes. She has to push, she said, so he gets gloves and long-sleeve shirts that keep his allergies in check. She sees the grind as necessary to ensure her husband survives.
“It is only because I am here that he is alive,” she said matter-of-factly. “They would've let him die.”

Outside the Washington State Penitentiary in Walla Walla, where inmates were holding a food strike in June to protest health and safety concerns, including food safety, health care and fears of COVID-19. (Ted S. Warren/AP)
Prisons budgets millions short
Darrell Cook, now 62, is increasingly representative of the aging prison population. The average age of a prisoner in Washington is nearly 40, and costs are rising.
Inmates are more likely than the public at large to have chronic medical conditions, yet the money allocated for their health care is significantly lower than would be spent if they were enrolled in a public insurance program like Medicaid, in which 86% of Washington prisoners enroll after release.
“We don't spend a comparable amount of money on the health care of people in jails and prisons as we would spend for those people when they're in the community,” said Stern, the former medical director, speaking generally.
“If you're underfunded … it’s just impossible to imagine that you can deliver constitutionally adequate care,” the correctional health care consultant continued.
To cut costs, prisons often “downshift” work from properly qualified providers to those with lesser credentials, Stern said. Most often, that means giving work that should be done by registered nurses, who generally have a bachelor’s degree in nursing, enabling them to direct treatment. Instead, the work goes to licensed practical nurses, most of whom have undergone a one-year certificate program.
“Not only is it beyond their legal scope of license … but it's also dangerous, for obvious reasons,” Stern said. “But it's done for financial reasons because LPNs are much less expensive than RNs or physicians.”
Beyond medical staff, the department can’t ensure officers are available to take ill inmates to hospitals or monitor inmates in a mental health crisis. Even with $3 million annually in additional funding, prison system leaders say they still lack the money to meet the growing medical and mental health needs of the incarcerated population.
The system is also antiquated, continuing to rely on paper medical records. Bankers boxes trail inmates moving from facility to facility. Chronically ill inmates clutch copies of their prescriptions and doctor’s orders as they’re bused around the state.
Darrell Cook, convicted in the mid-1990s of rape and, separately, murder, has seen his health falter, nearly dying after falling into anaphylactic shock due to an emergent allergy. He began to ask for a special diet to help with his allergy and saw his condition improve once a new medical director took over at the Monroe Correctional Complex. (Washington Department of Corrections)
When told of the financial constraints facing the department, Suzanne Cook hears a poor excuse.
“DOC has built into their own idea of themselves,” she said, “because they’re under this financial strain, they have to do what they have to do, even if it is torturing people.”
The culture of dehumanization in prison is infectious, says Washington, the former teen inmate, who is now 39. Through the mentoring of older prisoners, he found his place in society and his purpose in the life he’s enjoyed since July 9, 2019, decarceration.
Despite broad sentiment that American justice systems incarcerate too many people for too long, sentencing practices haven’t changed appreciably in the past decade. Washington state prisons remain at capacity and by some measures are among the nation’s most crowded.
Like many parolee activists still under the department’s authority, Washington worries he’ll face retaliation but sees his advocacy as a duty. He hopes the upswell in activism surrounding criminal justice reform will result in decarceration and prison reform, but sees no cause for optimism in the department’s COVID-19 response or timid steps toward reform.
“What we're seeing is more of the same,” he said. “We’re still being met with the same runaround.”

Suzanne Cook is cautiously optimistic about the health of her husband, Darrell, but she worries that his June transfer from Monroe back to Walla Walla, where the 62-year-old’s spate of near-fatal episodes began, may place his health back at risk. (Suzanne Cook)
This is the first in a three-part series on prison health. Next: Advocates and a state ombuds office say the DOC is missing opportunities to diagnose cancer in its earliest stages, and not treating patients already diagnosed with cancer.
